
 £
£
We use cookies to improve your experience. By accepting you agree to our cookie policy

By Caroline J Davies

Caroline J Davies is a physiotherapist specialising in Pain Reprocessing Therapy.
Whenever I write about CRPS, I feel an extra sense of responsibility to get things right and not to provide misleading hope. I understand, from a year as a senior physiotherapist at one of the national CRPS centres, how everything is harder and more difficult with CRPS. So, I am anxious to make two clarifications before continuing.
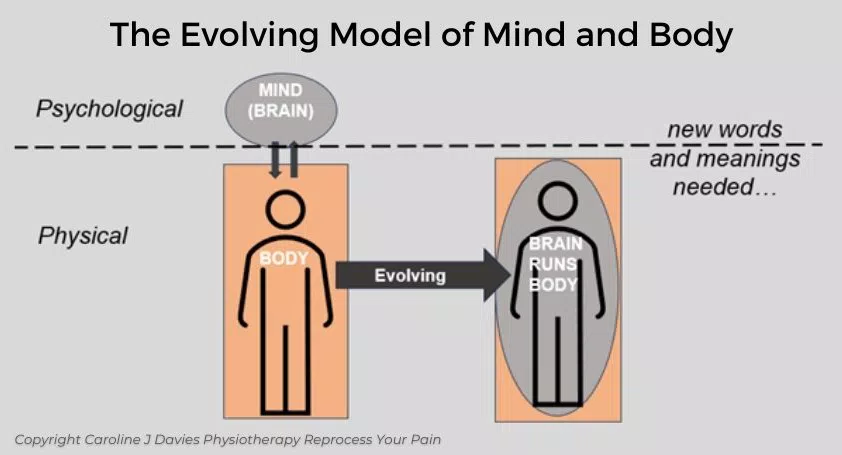
We tend to use the terms, “physical”, to describe problems within our bodies, and “psychological”, to describe problems within our minds (brains), as shown below, in the separated mind and body model to the left. As we come to understand how our brains predict almost all of our daily bodily (physical) experiences, including pain, we need new words, meanings and models; these could help our brains be more open to promising new therapies.
From the first moment we started to develop a brain and nervous system, about 6 weeks after conception [iii], we have been “recording” our experiences, both physical (what we did) and sensory (how we felt). From the daily repetitive tasks, like brushing our teeth or eating our breakfast, to the most physically or emotionally painful experiences, our brains made careful notes of them all.
Our brains play back these “recordings” or predictions for many reasons: to protect us by always being one step ahead of us; to save us energy by not having to process every physical sensation from the body in real time; and to help us become highly skilled at multiple tasks. Our brains have created our very own virtual reality world with many survival advantages, but some serious downsides.
Our brains’ predicted programmes are a bit like an old tape collection (recorded songs); some, you would never want to hear again, and others, you would do anything to hear one more time. What you would never want, would be the same bad tape playing over and over again. And that is what happens with our predicted pain recordings.
Although that sounds like very bad news, the good news is that, while not straightforward, we can learn how to record over the bad tapes.
I believe, the newer and promising treatments for CRPS and other types of pain, are working because they change the brain’s predicted pain programmes.
Like a restart or reboot for your computer, Scrambler Therapy uses surface skin electrodes to feed in multiple “normalising” sensory feelings from your body to your brain. This normal feedback is missing when you have CRPS. Scrambler Therapy is deservedly starting to attract interest from mainstream medicine. [iv]
Cognitive Multisensory Rehabilitation (CMR) is being trialled at the national CRPS centre in Bath [v]. This therapy also feeds in new sensory data to your brain, by sitting, for example, with your feet on a soft rug and noticing any normal or safe sensations you can find. Like Scrambler Therapy, this resets your brain’s predictions, reducing the CRPS symptoms.
Pain Reprocessing Therapy (PRT) helps you to unlearn your brain’s predictions or unconscious habits of pain. Understanding the new science of pain, is a key part of the therapy. Along with reprocessing your pain, you might explore potential causes and/or meanings of your pain, as well as processing any emotions arising around this. [vi] Interest and use of PRT for CRPS is expanding.
It feels like we need a new playlist of treatments for CRPS, as well as a new pain-free playlist for our brains.
The remaining questions I have now are: which treatments can change our brains the quickest, have the least side effects and are the most accessible, to reduce pain, return movement and normal sensations for people with CRPS? Are combinations of the different therapies more effective than one on its own?
See reprocessyourpain.co.uk for expanded articles on the above topics. I am a pain physiotherapist treating people with CRPS and chronic pain, in person and online.
[i] https://www.sciencefocus.com/the-human-body/how-your-brain-creates-pain-and-what-we-can-do-about-it
[ii] Hutchinson, J. B., & Barrett, L. F. (2019). The Power of Predictions: An Emerging Paradigm for Psychological Research. Current Directions in Psychological Science, 28(3), 280-291. https://doi.org/10.1177/0963721419831992 (Original work published 2019)
[iii] https://www.neurosciencefoundation.org/post/brain-development-in-fetus
[iv] https://www.painnewsnetwork.org/stories/2023/8/1/most-pain-patients-get-substantial-relief-from-scrambler-therapy.
[v] Batalla, M. A. P., & Lewis, J. S. (2024). Cognitive Multisensory Rehabilitation, a novel approach for Complex Regional Pain Syndrome: case series. Physiotherapy Theory and Practice, 1–15. https://doi.org/10.1080/09593985.2024.2393213
[vi] Ashar YK, Gordon A, Schubiner H, Uipi C, Knight K, Anderson Z, Carlisle J, Polisky L, Geuter S, Flood TF, Kragel PA, Dimidjian S, Lumley MA, Wager TD. Effect of Pain Reprocessing Therapy vs Placebo and Usual Care for Patients With Chronic Back Pain: A Randomized Clinical Trial. JAMA Psychiatry. 2022 Jan 1;79(1):13-23. doi: 10.1001/jamapsychiatry.2021.2669. PMID: 34586357; PMCID: PMC8482298.
We use cookies to improve your experience. By accepting you agree to our cookie policy